|
Oregon Advance Health Care Directive (Living Will) Form |
Oregon Advance Health Care Directive (Living Will) Form acts as direct communication between you, your Health Care Representative(s), and your Health Care Provider(s). When filling out this document, you will have the ability to solidify your feelings regarding basic scenarios involving medical treatments and interventions during traumatic medical emergencies or an end-of-life event. Additionally, you can directly report what you wish or do not wish employed regarding your treatment, address personal or religious concerns, and even set boundaries and limitations on a case by case basis. Keep in mind, you also retain the ability to revoke the representative powers you designate to your Health Care Representative at any time by issuing a written revocation or simply drafting and executing this directive with updated information.
Laws – ORS Chapter 127
How to Write
Download: Adobe PDF, Microsoft Word (.docx)
1 – Download The Advance Health Care Directive From This Page
Determine the file version best suited for your software environment from the “PDF” or “Word” buttons under the image.
2 – Your Identity Must Be Presented Before Declaring Your Health Care Representative
The first step in documenting your needs and aversions in this directive will be to attach your identity to this paperwork by attending the empty lines near the end of the page titled “Part A.” Locate the empty line just above the label “(Name)” then furnish your first, middle, and last name to this space. 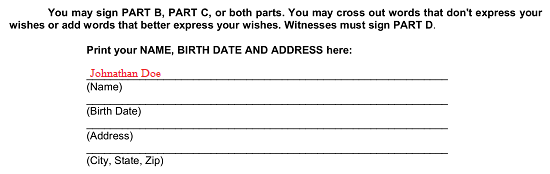 Two items will work together in this paperwork to verify it is your directive if necessary. The first is your birthday and this should be entered as a full calendar date on the blank line designated “(Birth Date).”
Two items will work together in this paperwork to verify it is your directive if necessary. The first is your birthday and this should be entered as a full calendar date on the blank line designated “(Birth Date).” 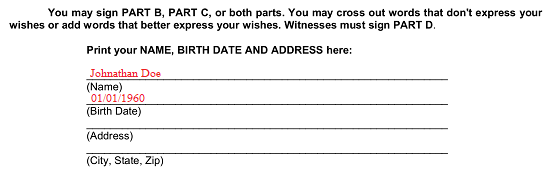 The second item that will aid in verifying the status of this paperwork will be your address as it is listed on your I.D. (i.e. State Driver’s License). Two lines “(Address)” and “(City, State, Zip)” are included here so you may easily record this material in a presentable manner.
The second item that will aid in verifying the status of this paperwork will be your address as it is listed on your I.D. (i.e. State Driver’s License). Two lines “(Address)” and “(City, State, Zip)” are included here so you may easily record this material in a presentable manner.  Before we move on to the next section, take a moment to determine then report how long you would like this directive to remain an active and accurate guide to your wishes when you can no longer communicate in a meaningful way. The sentence near the bottom of this document starting with the phrase “Unless Revoked Or Suspended…” will need your initials on the blank space to the left of one of the statements underneath it. Thus, if you wish this directive to be an active representation of your wishes for the rest of your life, then initial the line attached to the term “My Entire Life.”
Before we move on to the next section, take a moment to determine then report how long you would like this directive to remain an active and accurate guide to your wishes when you can no longer communicate in a meaningful way. The sentence near the bottom of this document starting with the phrase “Unless Revoked Or Suspended…” will need your initials on the blank space to the left of one of the statements underneath it. Thus, if you wish this directive to be an active representation of your wishes for the rest of your life, then initial the line attached to the term “My Entire Life.”  If you prefer this directive naturally terminate in a number of years, then initial the blank line corresponding to “Other Period…” and fill in the line before the word “Years” with exactly how many years you wish this directive to remain effective for.
If you prefer this directive naturally terminate in a number of years, then initial the blank line corresponding to “Other Period…” and fill in the line before the word “Years” with exactly how many years you wish this directive to remain effective for.  The next page is titled “Part B: Appointment Of Health Care Representative.” Take a moment to review it, then once you have determined which party should be assigned the role of your Health Care Representative, declare it so by placing his or her full name on the blank line between the term “I appoint” and “As My Health Care Representative in the first statement under this section’s “Note” paragraph.
The next page is titled “Part B: Appointment Of Health Care Representative.” Take a moment to review it, then once you have determined which party should be assigned the role of your Health Care Representative, declare it so by placing his or her full name on the blank line between the term “I appoint” and “As My Health Care Representative in the first statement under this section’s “Note” paragraph.  The next two available lines (following the words “My Representative’s Address Is”) will require the legal address of your Health Care Representative displayed on them. Confirm you have the correct information then furnish this requested content. You will also need to record his or her telephone number for the last line of this sentence
The next two available lines (following the words “My Representative’s Address Is”) will require the legal address of your Health Care Representative displayed on them. Confirm you have the correct information then furnish this requested content. You will also need to record his or her telephone number for the last line of this sentence  You should also considering naming an individual who can step in and assume the role of your Health Care Representative should your first choice be unable to assume this role after this document becomes effective but before you officially replace him or her. This “Alternate Health Care Representative” can only step in with the principal power you give through this document and only if you grant him or her the right to do so in the second statement provided. You will need to enter his or her name on the blank line preceding the term “As My Alternate Health Care Representative,” enter his or her address after the phrase “My Alternate’s Address Is…,” and supply his or her phone number(s) to the line attached to the words “And Telephone Number Is” at the end of this sentence.
You should also considering naming an individual who can step in and assume the role of your Health Care Representative should your first choice be unable to assume this role after this document becomes effective but before you officially replace him or her. This “Alternate Health Care Representative” can only step in with the principal power you give through this document and only if you grant him or her the right to do so in the second statement provided. You will need to enter his or her name on the blank line preceding the term “As My Alternate Health Care Representative,” enter his or her address after the phrase “My Alternate’s Address Is…,” and supply his or her phone number(s) to the line attached to the words “And Telephone Number Is” at the end of this sentence. 
3 – Discuss Any Limits To Your Agent’s Powers Then Address Some Basic Definitions
Later, in Part C, you will have the opportunity to address some specific scenarios and discuss what you wish done when are reliant on your Health Care Representative to communicate your wishes in treatment, care, or medical procedures. If there are any conditions or limits that should be set in place regarding the extent of the principal power you are designating to this Health Care Representative, then you must document them in the first article in Part B. Two blank lines in article “1. Limits” expects you to directly express “Special Conditions Or Instructions” that will apply to your Health Care Representative directly. This may take the form of conditional statements or direct instructions to him or her, you may add as much space as you like, or you may attach a document that you name in this area.  If you have issued a Health Care Directive or something of equal power of instruction to your Physician(s), then initial the blank space under the words “Initial If This Applies.” If you have not delivered any such directive to your Physicians or Health Care Providers, you may leave this line unmarked.
If you have issued a Health Care Directive or something of equal power of instruction to your Physician(s), then initial the blank space under the words “Initial If This Applies.” If you have not delivered any such directive to your Physicians or Health Care Providers, you may leave this line unmarked.  Another topic that will be dealt with in Part B will be in article “2. Life Support.” If you intend for your Health Care Representative(s) to decide whether or not keep you alive through life support machinery (when this is the only way you will live), then you must initial the blank line in this section. Do not initial this statement if you do not wish your Health Care Representative to have this power. In the example below, the Health Care Representative will be able to make decisions regarding the Principal’s (Your) life support because it is initialed by the issuer of this document.
Another topic that will be dealt with in Part B will be in article “2. Life Support.” If you intend for your Health Care Representative(s) to decide whether or not keep you alive through life support machinery (when this is the only way you will live), then you must initial the blank line in this section. Do not initial this statement if you do not wish your Health Care Representative to have this power. In the example below, the Health Care Representative will be able to make decisions regarding the Principal’s (Your) life support because it is initialed by the issuer of this document.  The final topic in part B will be “3. Tube Feeding.” If you wish your Health Care Representative to decide whether or not your nutrients and liquids should be delivered through a tube when (or if) you are unable to chew/swallow then you must initial the blank line attached to the words “My Representative May Decide…” If you do not wish your Health Care Representative to have the power of making this decision, then do not initial this statement. In the example below, the Health Care Representative will have the ability to decide whether the Issuer or Principal of this document should receive nutrients/liquids in this manner because this statement is initialed by the Issuer (Principal) of this document.
The final topic in part B will be “3. Tube Feeding.” If you wish your Health Care Representative to decide whether or not your nutrients and liquids should be delivered through a tube when (or if) you are unable to chew/swallow then you must initial the blank line attached to the words “My Representative May Decide…” If you do not wish your Health Care Representative to have the power of making this decision, then do not initial this statement. In the example below, the Health Care Representative will have the ability to decide whether the Issuer or Principal of this document should receive nutrients/liquids in this manner because this statement is initialed by the Issuer (Principal) of this document.  Now, for Part A and Part B to become effective and therefore respected as a representation of your wishes, you must sign the blank line at the bottom of the page labeled “Signature Of Person Making Appointment.”
Now, for Part A and Part B to become effective and therefore respected as a representation of your wishes, you must sign the blank line at the bottom of the page labeled “Signature Of Person Making Appointment.”  Immediately after signing your name, enter the current date on the “Date Signed” line underneath your signature.
Immediately after signing your name, enter the current date on the “Date Signed” line underneath your signature. 
4 – Convey Your Wishes During Several Scenarios In Part C
Part C of this document will give you the opportunity to be a bit more specific regarding the power you are designating to your Health Care Representative. The first four articles will require you initial only one of the statements in each part to give make your wishes known. Start with article “1. Close To Death.” If you are near the end of your life and cannot communicate then decisions over whether to administer tube feeding or life support can be made through this document. In section A of this article, you can elect to receive your nutrients through a tube (if necessary) as part of life-prolonging treatment when you initial the first statement.  If only your Physician should decide whether to maintain your life by providing your body with nutrients and liquids through a tube or to cease any tube feeding you are receiving, then initial the second statement.
If only your Physician should decide whether to maintain your life by providing your body with nutrients and liquids through a tube or to cease any tube feeding you are receiving, then initial the second statement. 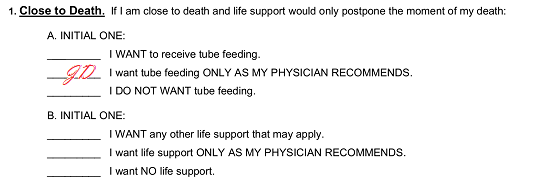 If you do not want your body maintained by receiving nutrients/liquids through a tube when you can no longer chew/swallow on your own, then initial the last statement in section A.
If you do not want your body maintained by receiving nutrients/liquids through a tube when you can no longer chew/swallow on your own, then initial the last statement in section A. 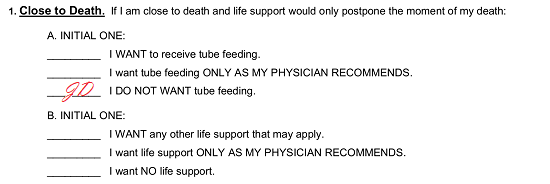 In section B of this article, we will discuss how you want life support to be viewed when you are “Close To Death” and can no longer communicate. A similar presentation as that in section B has been presented. If you wish your body to be kept alive by applying any life support technology (machines) to maintain body functions, then initial the first sentence in this section.
In section B of this article, we will discuss how you want life support to be viewed when you are “Close To Death” and can no longer communicate. A similar presentation as that in section B has been presented. If you wish your body to be kept alive by applying any life support technology (machines) to maintain body functions, then initial the first sentence in this section. 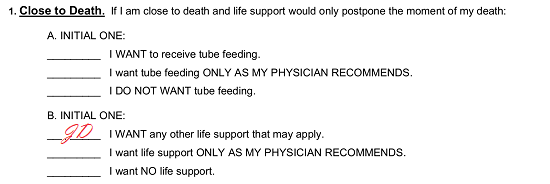 If the Physician is the only one who should decide when you should or should not be on life support, then initial the second sentence.
If the Physician is the only one who should decide when you should or should not be on life support, then initial the second sentence. 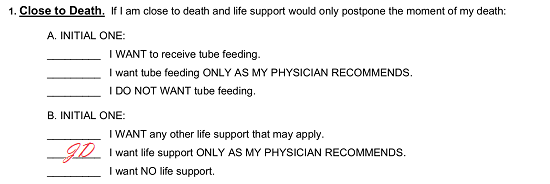 If you refuse to have your body kept alive by being dependent upon life support machines when you are “Close To Death” then initial the third sentence here.
If you refuse to have your body kept alive by being dependent upon life support machines when you are “Close To Death” then initial the third sentence here. 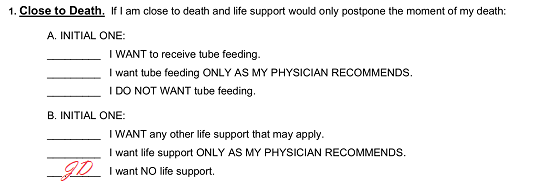 The second article here will want a definition to your wishes regarding tube feedings and life support when you have been officially diagnosed as “Permanently Unconscious.” Section A here will need your initial next to the first statement should you desire to be fed with the nutrients and liquids needed to sustain your body through a tube when there is little chance that you will wake up.
The second article here will want a definition to your wishes regarding tube feedings and life support when you have been officially diagnosed as “Permanently Unconscious.” Section A here will need your initial next to the first statement should you desire to be fed with the nutrients and liquids needed to sustain your body through a tube when there is little chance that you will wake up. 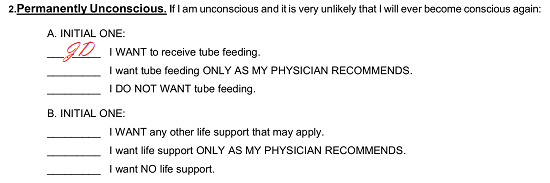 If you prefer that your Physician is the only entity able to determine when to administer tube feedings or when to withhold/cease tube feedings when you are “Permanently Unconscious” then initial the second statement.
If you prefer that your Physician is the only entity able to determine when to administer tube feedings or when to withhold/cease tube feedings when you are “Permanently Unconscious” then initial the second statement. 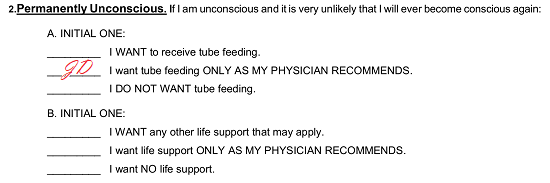 You may be against receiving nutrients or liquids through a tube if you are unconscious and will not wake up. If this is the case, then initial the third statement.
You may be against receiving nutrients or liquids through a tube if you are unconscious and will not wake up. If this is the case, then initial the third statement. 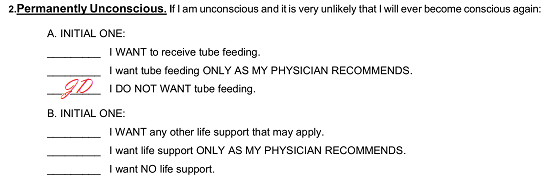 In section B of this article, we will discuss how life support should be included in your treatment when it is pronounced (by a Physician) that you will be unconscious for the remainder of your life. If you wish your body maintained by medical technology and placed on life support whenever necessary, then place your initials on the first statement.
In section B of this article, we will discuss how life support should be included in your treatment when it is pronounced (by a Physician) that you will be unconscious for the remainder of your life. If you wish your body maintained by medical technology and placed on life support whenever necessary, then place your initials on the first statement. 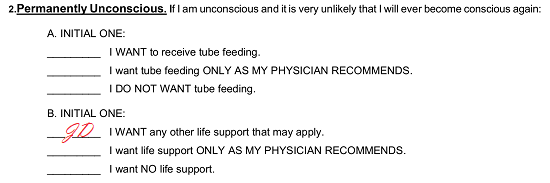 If the only party you wish to decide upon whether you receive, do not receive, or are taken off of life support when you’ve been diagnosed as “Permanently Unconcious,” then initial the second statement.
If the only party you wish to decide upon whether you receive, do not receive, or are taken off of life support when you’ve been diagnosed as “Permanently Unconcious,” then initial the second statement. 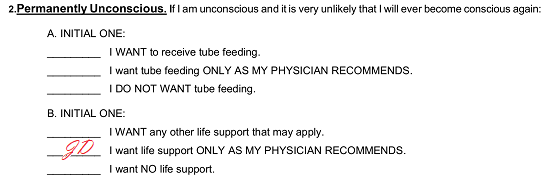 If you do not want life support machines administered when you are “Permanently Unconscious” then initial the third statement.
If you do not want life support machines administered when you are “Permanently Unconscious” then initial the third statement. 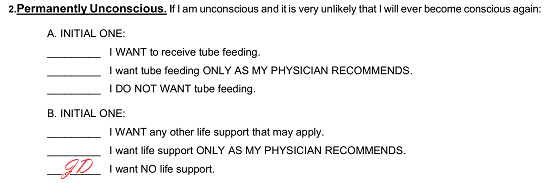 The third article, “3. Advanced Progressive Illness,” will ask your wishes on tube feedings and life support when you are struck down by a disease, “…Progressive Illness,” that will result in your death with very little hope for recovery and severe degradation in your ability to communicate, recognize people, remain conscious, or care for yourself. If you wish to have nutrients and liquids administered through a tube to maintain your life, then initial the first statement in section A here.
The third article, “3. Advanced Progressive Illness,” will ask your wishes on tube feedings and life support when you are struck down by a disease, “…Progressive Illness,” that will result in your death with very little hope for recovery and severe degradation in your ability to communicate, recognize people, remain conscious, or care for yourself. If you wish to have nutrients and liquids administered through a tube to maintain your life, then initial the first statement in section A here. 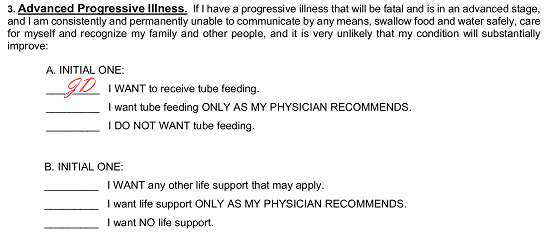 If you are unable to represent your wishes as a result of an “Advance Progressive Illness” and wish your Physician to be the person to decide when tube feedings should or should not be administered to you then initial the second sentence.
If you are unable to represent your wishes as a result of an “Advance Progressive Illness” and wish your Physician to be the person to decide when tube feedings should or should not be administered to you then initial the second sentence.  No tube feedings will be administered to maintain your life when you can no longer care for yourself during an “Advanced Progressive Illness” if you initial the last statement in section A of the third article.
No tube feedings will be administered to maintain your life when you can no longer care for yourself during an “Advanced Progressive Illness” if you initial the last statement in section A of the third article.  Section B will give you the chance to declare your position on life support when you have an “Advanced Progressive Illness” that has severely compromised your ability to survive and communicate. You may choose to have your life prolonged by machinery whenever necessary in such a case. If so, then initial the first sentence.
Section B will give you the chance to declare your position on life support when you have an “Advanced Progressive Illness” that has severely compromised your ability to survive and communicate. You may choose to have your life prolonged by machinery whenever necessary in such a case. If so, then initial the first sentence.  Your Physician will be the only one to represent your decision as to if you should or should not be placed on life support when a severe illness has crippled your ability to communicate when you initial the second sentence.
Your Physician will be the only one to represent your decision as to if you should or should not be placed on life support when a severe illness has crippled your ability to communicate when you initial the second sentence.  Initial the third statement in section B here if you do not want to be placed on life support even when it’s been deemed necessary to keep you alive during a serious debilitating disease.
Initial the third statement in section B here if you do not want to be placed on life support even when it’s been deemed necessary to keep you alive during a serious debilitating disease. 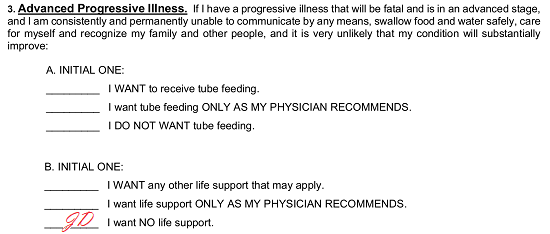 The next article here will specifically deal with “Extraordinary Suffering.” Here, use section A to pass along your wishes regarding whether you should be fed with a tube and receive liquids necessary to survive even under conditions where you are unable to represent yourself and are in a great amount of pain. Tube Feeding will be administered at the discretion of medical staff whenever necessary if you initial the first sentence.
The next article here will specifically deal with “Extraordinary Suffering.” Here, use section A to pass along your wishes regarding whether you should be fed with a tube and receive liquids necessary to survive even under conditions where you are unable to represent yourself and are in a great amount of pain. Tube Feeding will be administered at the discretion of medical staff whenever necessary if you initial the first sentence. 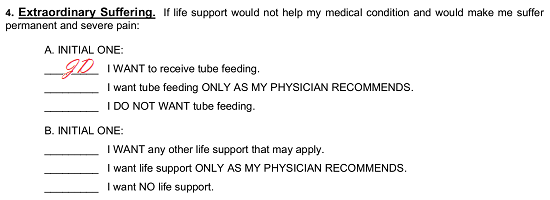 You may wish to limit the decision of placing you on or taking you off of tube feeding to your Physician. If you are in great pain that is permanent and cannot communicate and wish that only your Physician decides when it is appropriate to deliver liquids and nutrients through a tube to maintain your life, then initial the second statement.
You may wish to limit the decision of placing you on or taking you off of tube feeding to your Physician. If you are in great pain that is permanent and cannot communicate and wish that only your Physician decides when it is appropriate to deliver liquids and nutrients through a tube to maintain your life, then initial the second statement. 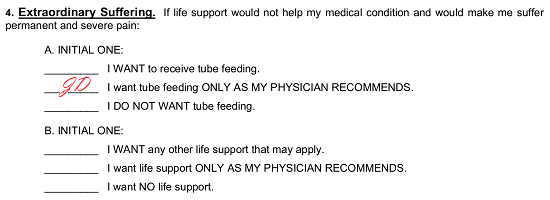 The third sentence will explicitly state that you “Do Not Want Tube Feeding” and will be taken as your wishes under these circumstances if you initial it.
The third sentence will explicitly state that you “Do Not Want Tube Feeding” and will be taken as your wishes under these circumstances if you initial it. 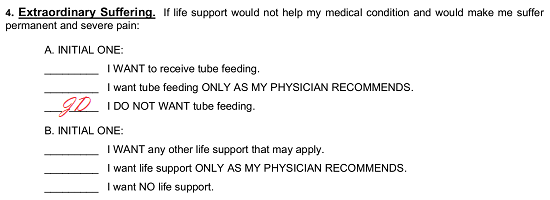 Section B of this article will also address the subject of being in “Extraordinary Suffering.” If you are unable to communicate and wish your life prolonged, even when in great pain, by life support machines if necessary, then initial the first sentence.
Section B of this article will also address the subject of being in “Extraordinary Suffering.” If you are unable to communicate and wish your life prolonged, even when in great pain, by life support machines if necessary, then initial the first sentence.  If only the Physician should have the decision-making power of maintaining your body with life support machines, then initial the next sentence.
If only the Physician should have the decision-making power of maintaining your body with life support machines, then initial the next sentence.  To declare that you do not want to be kept alive by life support machines when you are suffering greatly, initial the final sentence in section B and leave the previous two lines blank.
To declare that you do not want to be kept alive by life support machines when you are suffering greatly, initial the final sentence in section B and leave the previous two lines blank.  As a matter of convenience, you may automatically elect to die naturally if you initial the blank line in “5. General Instruction.” If you employ this tool, do not initial any of the directives above.
As a matter of convenience, you may automatically elect to die naturally if you initial the blank line in “5. General Instruction.” If you employ this tool, do not initial any of the directives above. 
5 – Personal Wishes May Be Included If Desired
In addition to the basic scenarios above, several other topics will be addressed by Part C. In article “6 Additional Care Or Instructions,” you will have the opportunity to address more personal issues that may be important during an end of life event. This article will be divided by topic and provide several sentences that have corresponding initial lines. You may initial as many of these statements that can be used as a description of how you want a topic handled. Let us review the first topic, “Dignity.” If you do not want your Medical Care Providers to engage in any actions (whether stated or unstated) with the intention of taking your life, then initial the first blank line under this heading. If you prefer Medical Personnel to work unimpeded even with this intention, then do not initial this statement.  Initial the second statement if you prefer that those in attendance (i.e. medical staff, family, etc.) act in accordance with your wishes whenever possible.
Initial the second statement if you prefer that those in attendance (i.e. medical staff, family, etc.) act in accordance with your wishes whenever possible.  The topic of “Comfort Care” will deal with your quality of life when you are near the end of it and cannot adequately communicate your needs. Each of the statements presented in this section will be a basic communication of your wants or needs when you are near the end of your life. In the example below, the Issuer of this directive or the Principal (You) wishes to engage in pain management procedures when necessary even if it will affect consciousness, to have favorite music played until the time of death, and to die at home if possible because these statements (1st statement, 4th statement, last statement) have been initialed. Read through this list, then initial each statement that accurately reflects your desires.
The topic of “Comfort Care” will deal with your quality of life when you are near the end of it and cannot adequately communicate your needs. Each of the statements presented in this section will be a basic communication of your wants or needs when you are near the end of your life. In the example below, the Issuer of this directive or the Principal (You) wishes to engage in pain management procedures when necessary even if it will affect consciousness, to have favorite music played until the time of death, and to die at home if possible because these statements (1st statement, 4th statement, last statement) have been initialed. Read through this list, then initial each statement that accurately reflects your desires.  This directive will have a statement pertaining to “Pregnancy.” If this topic applies and you are pregnant when you are suffering an end of life event then initial the blank line to indicate that you wish to receive tube feeding and life support machines to prolong your life under any circumstances if the embryo can go full term. Notice that this statement does not apply to the Principal in this example so it remains unapproved and will not apply.
This directive will have a statement pertaining to “Pregnancy.” If this topic applies and you are pregnant when you are suffering an end of life event then initial the blank line to indicate that you wish to receive tube feeding and life support machines to prolong your life under any circumstances if the embryo can go full term. Notice that this statement does not apply to the Principal in this example so it remains unapproved and will not apply.  The next section, “My Relationships With Family And Friend As My Death Approaches.” Each statement in this section will allow you to request certain things when you are near the end of your life. You may initial some of these, none of these, or all of these depending upon your preferences. This example states that the Principal will want to have people present as much as possible especially if “…It Seems That Death May Come At Any Time,” to have others by his or her side whenever possible, and to have pictures of his or her loved ones in the room and near the bed because the first, third, and last statements are initialed.
The next section, “My Relationships With Family And Friend As My Death Approaches.” Each statement in this section will allow you to request certain things when you are near the end of your life. You may initial some of these, none of these, or all of these depending upon your preferences. This example states that the Principal will want to have people present as much as possible especially if “…It Seems That Death May Come At Any Time,” to have others by his or her side whenever possible, and to have pictures of his or her loved ones in the room and near the bed because the first, third, and last statements are initialed.  The first eight statements in the section titled “What I Want My Loved Ones To Know” will follow a similar format as the two previous sections. Y0u must read through these statements then decide which ones best define any wishes, beliefs, or personal feelings and messages you want to be conveyed to them during a time when your life is near its end. The Principal below wishes loved ones to know that he or she loves them, forgives them for any past ills, and hopes they “Make Peace With Each Other” before his or her death if possible because the first, third, and fifth statements are initialed. Read through this list then initial any messages you wish passed on your behalf near the end of your life.
The first eight statements in the section titled “What I Want My Loved Ones To Know” will follow a similar format as the two previous sections. Y0u must read through these statements then decide which ones best define any wishes, beliefs, or personal feelings and messages you want to be conveyed to them during a time when your life is near its end. The Principal below wishes loved ones to know that he or she loves them, forgives them for any past ills, and hopes they “Make Peace With Each Other” before his or her death if possible because the first, third, and fifth statements are initialed. Read through this list then initial any messages you wish passed on your behalf near the end of your life.  You may also instruct your Health Care Representative on what to say if he or she is asked about how you wish to be remembered. If you do have a specific answer that you wish delivered, enter it after the statement “If Anyone Asks How I want to Be Remembered…” several empty lines have been produced in this area to accept your directive. If desired, you can also add more space or continue your instructions on an attachment that you name here.
You may also instruct your Health Care Representative on what to say if he or she is asked about how you wish to be remembered. If you do have a specific answer that you wish delivered, enter it after the statement “If Anyone Asks How I want to Be Remembered…” several empty lines have been produced in this area to accept your directive. If desired, you can also add more space or continue your instructions on an attachment that you name here.  If you have told someone what your funeral wishes are and wish your Health Care Representative to confer with them, then enter this person’s name on the blank line following the words “…Knows My Funeral wishes.”
If you have told someone what your funeral wishes are and wish your Health Care Representative to confer with them, then enter this person’s name on the blank line following the words “…Knows My Funeral wishes.” ![]() Furthermore, the next statement, “If There Is A Memorial Service…” allows you to spell out specific requests for any service held in your honor after death. Several blank lines have been supplied here for your use in providing any requests you may have.
Furthermore, the next statement, “If There Is A Memorial Service…” allows you to spell out specific requests for any service held in your honor after death. Several blank lines have been supplied here for your use in providing any requests you may have.  One final area has been supplied for your convenience. If you have any other instructions or directives you wish documented for your Health Care Representative or any other preferences, conditions, or opinions regarding your end of life care or scenarios where you are unable to represent yourself then place them in the “Other Instructions” section.
One final area has been supplied for your convenience. If you have any other instructions or directives you wish documented for your Health Care Representative or any other preferences, conditions, or opinions regarding your end of life care or scenarios where you are unable to represent yourself then place them in the “Other Instructions” section. 
6 – Document How Additional Health Care Relate To This Document Then Execute It
In article “7. Other Documents,” a definition as to how this document and other health care directives you’ve issued will interact. If you have a Health Care Power Of Attorney that is active and must remain active while this one is in effect, then initial the line attached to the statement “I Have Previously Signed…”  If you have issued a Health Care Power Of Attorney and intend to revoke it with the execution of this one then, initials the second statement.
If you have issued a Health Care Power Of Attorney and intend to revoke it with the execution of this one then, initials the second statement.  The last choice should only be initialed if you do not have another Health Care Power Of Attorney currently in effect. Initial the “I Do Not…” statement if this is the only Health Care Power Of Attorney that will be active at the time of execution.
The last choice should only be initialed if you do not have another Health Care Power Of Attorney currently in effect. Initial the “I Do Not…” statement if this is the only Health Care Power Of Attorney that will be active at the time of execution.  Lastly, a strict requirement Part C makes that must be satisfied is a call for your signature. The act of signing this document will place it in effect so that all its contents apply to your health care (and your Health Care Representative). Put this document in effect by signing the blank line labeled “Signature Of Person Giving Instructions” then immediately entering the current calendar date on the blank space labeled “Date Signed.”
Lastly, a strict requirement Part C makes that must be satisfied is a call for your signature. The act of signing this document will place it in effect so that all its contents apply to your health care (and your Health Care Representative). Put this document in effect by signing the blank line labeled “Signature Of Person Giving Instructions” then immediately entering the current calendar date on the blank space labeled “Date Signed.”  Upon successfully signing this directive, the Principal should give it to the Witnesses present at the time. Each one will need to read through “Part D: Declaration Of Witnesses.” There will be two signature areas consisting of the lines “Signature Of Witness,” “Printed Name Of Witness,” and “Date Signed.” Each Witness must verify his or her ability to qualify as a Witness and that the statements in this section are accurate by signing his or her name, printing his or her name, and dating his or her signature to the properly labeled lines in in the Witnessed By.”
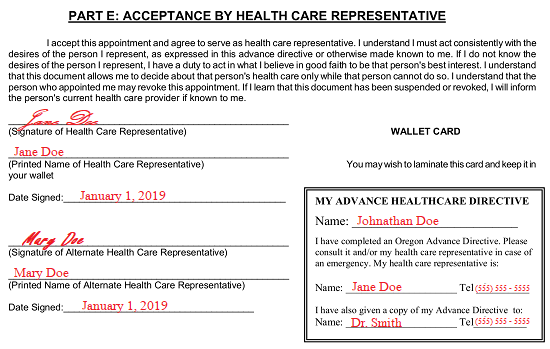
Upon successfully signing this directive, the Principal should give it to the Witnesses present at the time. Each one will need to read through “Part D: Declaration Of Witnesses.” There will be two signature areas consisting of the lines “Signature Of Witness,” “Printed Name Of Witness,” and “Date Signed.” Each Witness must verify his or her ability to qualify as a Witness and that the statements in this section are accurate by signing his or her name, printing his or her name, and dating his or her signature to the properly labeled lines in in the Witnessed By.” Each Health Care Representative named in this document must formally accept his or her responsibility to this role as it is defined here by attending to “Part E: Acceptance By Health Care Representative.” There will be enough room here for the Health Care Representative then the Alternate Health Care Representative to sign their names as an acknowledgment of their role then provide their printed names and signature dates (respectively).
Each Health Care Representative named in this document must formally accept his or her responsibility to this role as it is defined here by attending to “Part E: Acceptance By Health Care Representative.” There will be enough room here for the Health Care Representative then the Alternate Health Care Representative to sign their names as an acknowledgment of their role then provide their printed names and signature dates (respectively).  As a matter of convenience, a wallet card set to display your name then the names and phone numbers of your Health Care Representatives have been included. Fill it out then detach it and keep it in your wallet as a precaution.
As a matter of convenience, a wallet card set to display your name then the names and phone numbers of your Health Care Representatives have been included. Fill it out then detach it and keep it in your wallet as a precaution.